
Fire is an actuality of very low probability, but one of severe consequence. Once it starts to spread, fire moves quickly, producing an abundance of blinding toxic smoke. And smoke kills. If you think long and hard about each and every building in your town, the very last place you would want a fire to start is in your local hospital.

The
typical pendent sprinkler today (on the left) is a lighter and less-obtrusive
version of the 1970s vintage Hodgman chrome pendent sprinkler on the right.
No Easy Way Out
Hospitals are large places. Virtually everyone who has visited a friend or relative in a hospital has had a similar experience after leaving the visiting room-difficulty finding his way out. And this is under normal conditions. Consider others in the same hospital trying to exit or just move to a safe location under emergency conditions-patients who are sound asleep, patients who are not able to walk normally, those sedated, those in treatment, those in intensive care, the very old, newborn babies. No, a hospital or healthcare facility is most assuredly the type of standing structure in which we would never want to see the onset of fire.Certainly, architectural and design features of fire safety have evolved over time, and fire statistics have recorded a matching measure of success. Many hospital and healthcare facility fires are small and can be extinguished in the incipient stage, so that local fire departments are often unaware of those occurrences. With an increase in fire safety awareness, buffeted by stricter code enforcement, the number of such small, unreported fires has most likely risen over time.

The
abundance of mechanical components above this hospital ceiling gave an
installer no choice but to offset this cross-main. An auxiliary drain will
service the trapped piping downstream of the offset location.
However, despite the potential for fire within these buildings, when compared to other U.S. occupancies and structures, the overall fire record for healthcare facilities is remarkably low. This may be due to the high number of staff on hand, fire-resistive construction, the plethora of interior fire-retardant building materials, or the fact that combustible fuel load is very low in these facilities.
Cause and Origin
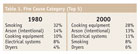
Today, roughly one-fourth of all healthcare facility fires begin in kitchens or rooms otherwise set aside for food preparation. Thirteen percent start in patient rooms, and about 8% of these fires originate in laundry areas. Fire, however, can ignite almost anywhere. Table 1 (Left Side) illustrates how the causes of reported fires have changed over a 20-year period in hospitals and healthcare facilities.Other, less prevalent causes of origin are almost too numerous to list. They include generators, air-conditioning equipment, various types of heating components, televisions, refrigeration equipment, incinerators and other items of medical equipment that are particular to hospitals, such as oxygen tanks. As improbable as it may seem, a number of fires in healthcare facilities have started when a patient simply didn’t move far enough away from an oxygen cylinder before attempting to light a cigarette. Improper storage or transfer of liquid oxygen, unsafe usage of tanks in kitchens and workshops, and smoking around oxygen (by patients or visitors) are real risks for healthcare agencies. They are not limited to just the patient rooms.

The lack of automatic sprinklers proved disastrous in a 1997 board-and-care fire in Harveys Lake, PA. That fire was started by the careless disposal of smoking materials inside a screened-in porch. Ineffective response by staff, coupled with the hampered evacuation capabilities of the residents, resulted in one gutted building and 10 fatalities. More recently, 18 people perished when they were trapped by flames this year in a hospital fire in Costa Rica. The cause was an apparent gas leak in an outpatient service area situated in the oldest part of the hospital-built 150 years ago. Dozens of survivors escaped by lowering themselves from windows using bed sheets.

A 6" underground feed will supply both a 4" fire sprinkler riser and the domestic water for this building addition.
The Code Compliance Debacle
Structures housing this nation’s healthcare operations are among the most heavily regulated in our history. If designing for a new hospital or new addition, the code documents that need to be investigated are far too numerous to mention. At last count, there are more than 60 NFPA documents alone that are applicable to healthcare facility occupancies. As the traditional healthcare landscape changes, the odyssey of code compliance becomes a never-ending journey. It’s a code-saturated playing field.The typical U.S. hospital must comply with local fire and building codes, state fire and building codes, various requirements scripted by state health department officials, one of the current model building codes, NFPA 101: Life Safety Code, the Americans With Disabilities Act (ADA) design guidelines, Health-Care Finance Administration (HHS/HCFA) life safety codes and the design guidelines of the Joint Commission for the Accreditation of Healthcare Organizations (JCAHO) Plant and Technology requirements.
This is a short list, which doesn’t include any interim policy changes implemented by the above-captioned agencies. Pending location and local jurisdiction intervention, the time spent conducting pre-construction, mid-construction and plan review meetings will vary considerably. In any case, documentation of such meetings and strategy sessions will mount into a veritable paper jungle.
Next month, in part two, I’ll wrap-up my discussion of code requirements and also address egress and fire suppression and equipment.