Within the history of the development of the drainage network design guides we now take for granted, there have been some celebrated differences of opinion. Some, of course, are recent, while others, despite dating from the mid-Victorian era, still have an impact on our design codes and general approaches to public health.
In London in 1854, one such major difference of opinion centered around the cholera epidemic in the Soho area of the city-at that time a poorer or "working class" section of the capital. The difference of opinion revolved around the mode of transmission of the epidemic-was the disease transmission waterborne or airborne?
Edwin Chadwick, as commissioner of the Board of Health, believed that the spread of the disease was airborne. In common with many Victorians, he believed that the disease spread through miasma and could be combated by improved ventilation.
Chadwick had been appointed to the post of assistant commissioner of the Poor Law Commission in 1832, and in 1839, he established the first sanitary commission to investigate a local epidemic in Whitechapel. This report was fundamental in formulating public opinion and provided a model for improved sanitation across the U.K., establishing Chadwick as a pioneer public sanitation reformer. Chadwick was convinced that living conditions were inexorably linked to the continuous epidemics sweeping the congested areas of British cities in the 1840s. His nationwide Report into the Sanitary Condition of the Labouring Population of Great Britain, published in 1842, was seminal. In many respects, Chadwick, an abrasive and goal-orientated campaigner and civil servant, was a product of his age-representing perhaps the best and worse elements of the Victorian public reforming ethic.
In 1847, Chadwick advocated the separation of sewage and drainage systems, and in the following year, he led a campaign for the introduction of the Public Health Act of 1848. Chadwick was appointed commissioner of the Board of Health from 1848 to 1854.
The concentration on miasma as a source of disease spread had the effect of generating extremely conservative building drainage and vent system design guidance, some of which survives to the present day.
The controversy was finally resolved by John Snow's ground-breaking investigation of the source of the cholera epidemic. Dr. Snow, an obstetrician with an interest in many aspects of medical science, had long believed that water contaminated by sewage was the cause of cholera. Through careful plotting of the sites of infection, a modern technique familiar to all "cluster" infection investigations, he was able to identify the source as the Broad Street pump used by many local residents. His proof was reinforced by his discovery that workers at a local brewery, who preferred their product or the brewery's own water supply to the public pump, were seemingly immune. Despite initial denials of his findings by the Board of Health, his work finally ended the discussion and led to a much greater emphasis on the provision of water treatment.
The Victorian obsession with odor as an indicator of disease, however, remained and permeated the drainage design process. The so-called two-pipe system, where gray and black water was segregated within the building drainage network, with each sector having its own dedicated vent stack connected to each individual appliance, remained the U.K. standard approach well into the 20th century, only giving way in the 1930s to the one-pipe system, still featuring a full vent system to each appliance. Then in the 1970s, the U.K. Single Stack System became standard, and later, it was the replacement of open vents with air admittance valves in the 1980s.
The recent spread of infection within multi-story buildings may, however, vindicate some of Chadwick's views. The recent SARS epidemic in Hong Kong is a case in point where it has now been established that the spread of the disease was influenced by both the design and maintenance level of the installed building drainage and vent system. At a presentation given to the Royal Society of Edinburgh in Dec. 2003, Dr. Martin Donaghy, clinical director of the Scottish Centre for Infection and Environmental Health, commented that "reports from Amoy Gardens indicate that spread accelerated once diarrhea had set in among those infected." In a multi-story building, it would be recognized that the appliance discharges, falling as an annular film, would result in the entrained airflow being effectively a mist of entrained airflow and water droplets thrown out into the airstream by any stack junction or discharging branch. In the case mentioned by Dr. Donaghy, this mist would consist of dilute diarrhea droplets. When this is combined with the known lack of trap seal maintenance, and in particular, trap seal loss in floor traps in bathroom areas including showers, extraction fans and high temperatures, it is clear that Chadwick's concerns as to miasma as a source of infection may well have been justified.
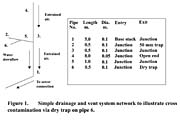
Thus, it would be instructive to model the possible effect of a dry trap in a shower cubicle fitted with an extraction fan whose operation might well be linked to the cubicle lighting. The vent system simulations developed at Heriot-Watt over many years will cope with this set of design constraints. Figure 1 illustrates an extremely simplistic network chosen to highlight the main features of the discussion. It is assumed that the trap on pipe 6 is dry and that the cubicle fan is operational from time zero. At the 10-second point in the simulation, a series of 6 litre w.c. flushes passes down the main stack; thereafter, the shower flow alone is present.
Thus, the simulation of likely system operation, including modeling of the effect of poor maintenance, can provide both a predictor of risk, and post event, a forensic analysis of failure.
Finally, 150 years later, Chadwick had a point: airborne contamination can be important. However, he missed the essential need to accept that more than one mechanism may be at work and that the prevention of miasma alone is insufficient.